All published articles of this journal are available on ScienceDirect.

Integrating Slow-paced Breathing into Pre-shot Routine: Acute Effects on Heart Rate Variability and Golf Swing Performance under Pressure
Abstract
Introduction/Background
Slow-Paced Breathing (SPB) is a reliable intervention for emotional regulation that facilitates autonomic stability. When integrated into Pre-Shot Routines (PSR) of golfers, SPB facilitates emotional regulation, sustains attentional stability under pressure, and ensures precise motor execution. However, the psychophysiological impacts of integrating SPB into PSR and their effects on performance outcomes have yet to be fully characterized across varying conditions.
Objectives
This study aims to examine the effects of SPB integrated with PSR (SPB+PSR) on swing performance and autonomic regulation.
Methods
This study used a within-subject, repeated measures design. Fifteen male golfers (aged 18–30) completed three protocols: PSR, SPB+PSR under control (non-pressure) conditions, and SPB+PSR under pressure. Autonomic activity (measured via RMSSD), heart rate, swing characteristics, and psychological states were recorded before and after the golf swing test.
Results
The SPB+PSR protocol showed significantly higher RMSSD and lower heart rate responses than PSR alone (p-value < 0.05). Under pressure, SPB+PSR resulted in better swing distance but increased lateral deviation as compared to the normal condition. Although golfers reported enhanced mental clarity and relaxation when performing SPB+PSR, their confidence decreased under pressure.
Discussion
The increased RMSSD observed in the SPB+PSR protocol indicates a reduction in physiological stress and an enhancement of parasympathetic activity. However, the decrease in shot accuracy under pressure suggests that SPB's efficacy in improving performance outcomes may be limited. It is plausible that moderate arousal impaired fine motor control and decreased self-confidence, thereby attenuating the physiological benefits of the breathing intervention.
Conclusion
The SPB+PSR protocol enhances autonomic regulation and psychological readiness in male golfers. While this protocol improves swing performance, its efficacy in maintaining shot accuracy diminishes under pressure. Consequently, integrating SPB into PSR may help golfers manage their mental state and motor control, though additional training may be needed to maintain performance in high-demand, unpredictable environments.
1. INTRODUCTION
Golf demands high levels of movement precision and consistency, requiring players to maintain an optimal psychophysiological state throughout each swing. The initial shot of a hole, primarily the driver swing, is highly susceptible to psychological pressure during competition. Under high-pressure conditions, golfers may experience intrusive thoughts and increased conscious processing, which can disrupt decision-making and swing mechanics [1]. To alleviate these detrimental effects, most golfers employ Pre-Shot Routines (PSR), including strategic planning, visualization, and self-talk to achieve psychological readiness and focus attention on shot demands [2, 3]. While the benefits of PSR for anxiety and shot accuracy have been documented [4, 5], the specific physiological mechanisms involving vagal modulation remain underexplored.
The PSR protocol requires a reliable mechanism for physiological self-regulation, which is effectively achieved through Slow-Paced Breathing (SPB). Typically, SPB is practiced at a diaphragmatic rhythm of 4-6 breaths·min−1. By lengthening the exhalation phase, this technique maximizes baroreflex sensitivity, thereby elevating vagal tone [6, 7]. The shift toward parasympathetic dominance can be detected by the Root Mean Square of Successive Differences (RMSSD), which is a reliable measure of vagal-mediated Heart Rate Variability (HRV) in sporting contexts [8]. The link between this physiological shift and golf performance is based on vagal tank theory, which relies on the neurovisceral integration model [9]. Increased vagal tone facilitates higher-order functions in the prefrontal cortex, which is essential for maintaining attentional stability and emotional regulation. By stabilizing the cardiovascular system, SPB acts as a buffer against the high arousal states that often disrupt fine motor control. This state of physiological calm keeps the golfer within an optimal psychophysiological zone, ensuring the swing remains governed by automaticity rather than conscious, anxious interference [8].
Despite these theoretical links, evidence regarding the psychophysiological impact of combining SPB with PSR remains not fully characterised across varying conditions. It is unclear whether the vagal enhancement induced by SPB effectively buffers motor execution from the detrimental effects of stress. To address this, the present study evaluated the effects of an integrated SPB+PSR protocol under pressure and control conditions compared to a standard PSR. It was hypothesized that both SPB+PSR integrated conditions would elicit higher RMSSD values and superior swing performance compared to the standard PSR, with the physiological synergy of the SPB+PSR protocol being maintained even under pressure.
2. METHODOLOGY
2.1. Study Design
This study used a within-subject, repeated-measures experimental design to investigate how different pre-shot routines (PSR) affect psychophysiological responses and golf swing performance. Participants followed a standard PSR protocol using normal breathing against an integrated Slow-Paced Breathing (SPB). The SPB-integrated PSR interventions were performed in two distinct settings: non-pressure condition (SPB+PSR [Normal]) and pressure condition (SPB+PSR [Pressure]). This study was approved by the Thammasat University Ethics Review Sub-Committee (COA. 064/2565), and all participants provided written informed consent before taking part.
An a priori power analysis was conducted using G*Power 3.1 for repeated-measures ANOVA (α = 0.05, power = 0.95). Based on large HRV effects reported in a comparable experimental design (f = 0.45) [8], and consistent with meta-analytic evidence on slow-breathing interventions [10], the minimum required sample size was 10 participants. To account for potential dropouts, a total of 15 participants were recruited for this pilot study.
2.2. Participants
Participants were recruited between November 1, 2022, and March 30, 2023, through announcements at golf clubs and training academies. Eligible participants were male golfers aged 18 or older who held amateur or professional status, competed in at least 3 tournaments per year, and maintained a handicap between 0 and 5. Participants were excluded if they had cardiovascular, respiratory, or musculoskeletal disorders within the previous 3 months, or if they had acute illness or injuries that could hinder their ability to complete the study protocol. A total of 15 male golfers met these criteria and were enrolled, reporting an average of 8.57 years of competitive experience and 5.80 tournaments per year. On average, participants practiced at driving ranges 4.87 ± 0.92 days per week and played on golf courses 2.33 ± 1.73 times per week.
2.3. Procedure and Data Acquisition
The experiments took place in a distraction-free, climate-controlled laboratory maintained at 23–25°C. After attaching ECG electrodes to monitor physiological changes, participants completed an initial 5-minute seated rest to establish baseline heart rate (HR) and HRV. Afterward, they followed a standardized warm-up consisting of 5 minutes of light movement and 10 minutes of progressive swings, concluding with a final 5-minute seated rest. As shown in Figure 1, HR and HRV data were collected during two resting periods (Baseline and Resting+SPB), three golf swing conditions (PSR, SPB+PSR [Normal], and SPB+PSR [Pressure]), and three post-task phases. Each post-task phase began with a psychological readiness self-report, followed by HR and HRV monitoring.
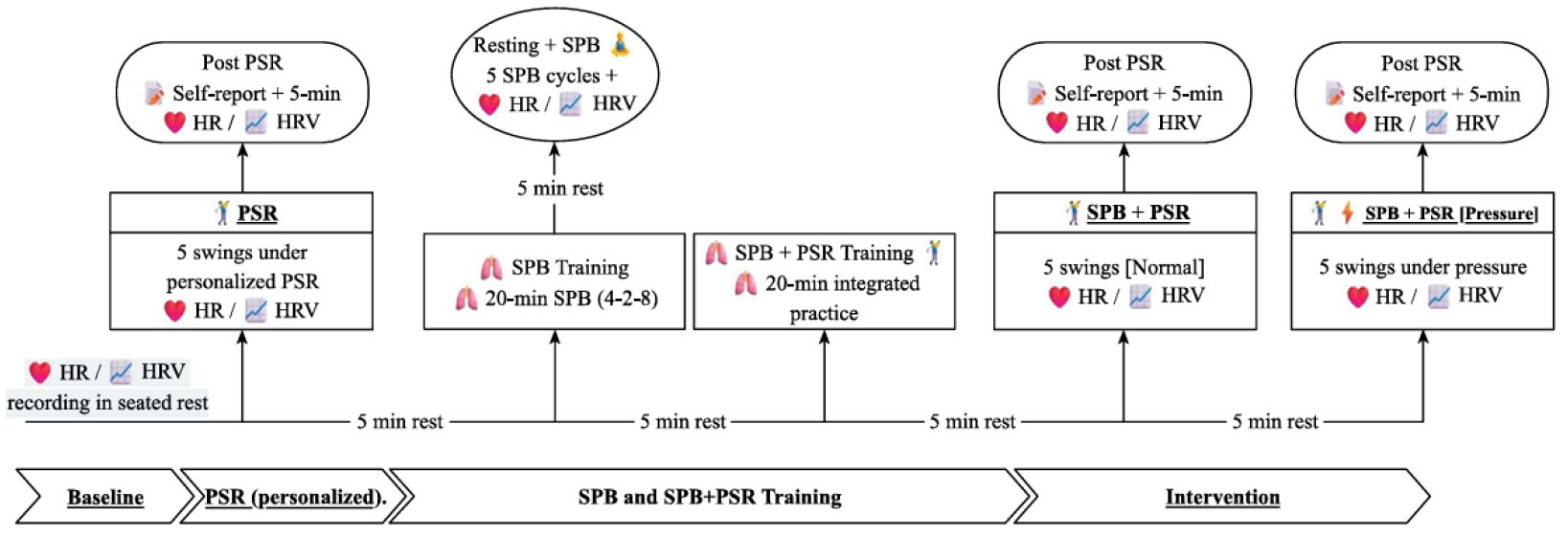
Flow chart of the experimental protocol.
To simulate the psychological stress of competition, participants were informed before the pressure-induced condition that their performance would be recorded, ranked, and compared against others, with rewards offered to the top three performers. While participants could only view their own results, this protocol was designed to elicit moderate psychological stress rather than the high-intensity pressure of a professional tournament. To confirm the effectiveness of this induction, we conducted a manipulation check using perceived pressure, ensuring that the protocol successfully shifted participants into a moderate state of stress without reaching debilitating levels.
2.4. Breathing intervention and Pre-shot Routine
The SPB technique utilized a diaphragmatic 4-2-8 breathing pattern (inhale-hold-exhale), initially guided by the Breathe+® mobile application. After verifying that participants could perform the technique correctly, they completed a 5-minute baseline rest followed by five monitored SPB cycles.
Next, participants integrated the SPB into their PSR at two specific stages: (1) during target visualization and (2) immediately before the backswing. Before moving to the golf swing evaluations, each golfer had to demonstrate a consistent breathing rhythm within their sequence. No external feedback or application guidance was provided during the swing tests. The participants followed their own PSR protocol to ensure the breathing felt natural and integrated. To maintain high procedural validity, a sport psychology expert (SK.) monitored all sessions to ensure every step was executed accurately.
2.5. Swing Performance Recording
Golf swing performance was evaluated using a FlightScope Xi Tour launch monitor (FlightScope, South Africa), positioned 2.5 meters away from the hitting area. Using their own drivers and standardized Bridgestone X5 golf balls, participants performed five swings from a standard tee height and mat, with a 30 to 60 second rest between trials. Following each trial, participants reviewed their clubhead speed, carry, and total distance, and lateral deviation via the launch monitor display. These parameters were recorded for every trial and averaged for data analysis.
2.6. Heart Rate (HR) and Heart Rate Variability (HRV) Monitoring
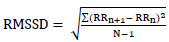
HR and HRV were recorded continuously throughout all procedures, including resting and golf swings. Data were collected using the Medicom Egoscop (Medicom, Russia), which captures inter-beat intervals (IBIs) in milliseconds (ms) and transmits the data wirelessly to a computer. To ensure signal integrity and minimize motion artifacts during the swing, the skin was shaved and cleaned with alcohol wipes, and two electrodes were attached to the ventral aspects of the left and right forearms (5–8 cm from the wrists) and secured with Coban bandages. HRV was measured using the RMSSD value, calculated using Eq. (1) [11]:
 (1)
(1)
where RRₙ represents successive normal-to-normal intervals, and N denotes the total number of intervals. Following the removal of all RR intervals exceeding 1,000 ms, only data points requiring less than 5% correction were retained for analysis. The RMSSD was subsequently averaged across the five swing trials of each experimental condition. Finally, HR and percentage of maximum heart rate (%HRmax) were calculated using Eq. (2) [12]:
 (2)
(2)
2.7. Self-report Psychological Readiness
Following the golf swing tests, participants completed a questionnaire evaluating state-based indicators consisting of performance readiness and emotional regulation across three dimensions. First, mental clarity assesses how participants feel about their mental preparedness before the shot attempt through the question: “How mentally clear and ready did you feel to aim and execute your shot?” Second, participants rated their muscle relaxation state before initiating their swing by answering: “To what extent did your body feel physically relaxed before swinging?” Third, self-confidence was evaluated by asking, “How confident did you feel in making a successful shot?” regarding the feeling of success during the swing shot. All responses were recorded on a 5-point Likert scale (0 = not at all, 4 = extremely). Content validity was evaluated by expert review (two sport psychologists and three certified golf coaches). The results confirmed that all items were clear and relevant to participants.
2.8. Data Analysis
The data were analyzed using R Studio (Version 2024.12.1; Posit Cooperative). Normality and sphericity assumptions were assessed using Shapiro-Wilk and Mauchly’s tests, respectively. The Greenhouse-Geisser epsilon correction was applied to deal with the violation. Comparisons among interventions were performed using a repeated-measures ANOVA with Bonferroni-adjusted post hoc tests. To assess psychological readiness, the Friedman test was employed. Effect sizes were reported as partial eta squared (eta-squared) for ANOVA and Hedges' g for pairwise comparisons. To account for potential bias in small sample sizes, g was adjusted using Eq. (3) [13]:
 (3)
(3)
Interpretation of g followed Cohen’s conventional thresholds: small (0.2), medium (0.5), and large (0.8) [14]. All analyses were determined at p-values less than 0.05.
3. RESULTS
3.1. Effects on Autonomic Regulation
Table 1 shows that RMSSD was significantly higher during the Resting+SPB condition compared with Baseline, PSR, Post SPB+PSR [Normal], and Post SPB+PSR [Pressure] (Hedges’ g: 1.03–1.47, p-value < 0.05). Moreover, the SPB+PSR intervention under both normal and pressure conditions showed significantly greater RMSSD values than the PSR alone (Hedges’s: 1.02-1.03, p-value < 0.05).
| Condition | Mean ± SD | 95% CI | Significant Comparisons | |||
|---|---|---|---|---|---|---|
| Paired Condition | p-value | Hedges’g | 95% CI of g | |||
| Baseline | 32.29 ± 10.48 | 26.48–38.09 | - | - | - | - |
| Resting+SPB | 47.78 ± 11.19 | 41.58–53.98 | Baseline | 0.031 | 1.03 | 0.41 to 1.66 |
| PSR | 30.72 ± 11.14 | 24.55–36.90 | Resting+SPB | 0.005 | -1.27 | -1.95 to -0.59 |
| Post PSR | 35.23 ± 13.76 | 27.61–42.85 | - | - | - | - |
| SPB+PSR [Normal] | 42.68 ± 18.08 | 32.67–52.69 | PSR | 0.035 | 1.02 | 0.39 to 1.64 |
| Post SPB+PSR [Normal] | 34.75 ± 11.53 | 28.37–41.13 | Resting+SPB | 0.025 | -1.06 | -1.70 to -0.43 |
| SPB+PSR [Pressure] | 41.24 ± 15.93 | 32.41–50.06 | PSR | 0.033 | 1.03 | 0.40 to 1.65 |
| Post SPB+PSR [Pressure] | 31.37 ± 8.06 | 26.91–35.84 | Resting+SPB | 0.001 | -1.47 | -2.20 to -0.74 |
Note: Values are presented as mean ± SD with 95% confidence intervals (CI). ANOVA results: F(7,98) = 7.17, p-value < 0.001, η2p = 0.34. PSR = pre-shot routine; SPB = slow-paced breathing.
Furthermore, results showed significantly lower HR (g: 1.09–2.83, p-value < 0.05) and percentage of maximum heart rate (%HRmax) (Hedges’g: 1.09-2.93, p-value < 0.05) during the Resting+SPB condition compared with all other conditions. While HR and %HRmax increased during golf swings, these values dropped to levels slightly below baseline during subsequent resting periods (Tables 2 and 3).
| Condition | Mean ± SD | 95% CI | Significant Comparisons | |||
|---|---|---|---|---|---|---|
| Paired Condition | p-value | Hedges’g | 95% CI of g | |||
| Baseline | 78.58 ± 6.65 | 74.90–82.27 | - | - | - | - |
| Resting+SPB | 73.88 ± 4.44 | 71.42–76.34 | Baseline | 0.038 | -1.01 | -1.63 to -0.38 |
| PSR | 104.82 ± 13.77 | 97.19–112.44 | Baseline | <0.001 | 2.18 | 1.25 to 3.11 |
| Resting+SPB | <0.001 | 2.44 | 1.43 to 3.44 | |||
| Post PSR | 82.91 ± 10.65 | 77.01–88.80 | PSR | <0.001 | -2.88 | -4.03 to -1.73 |
| Resting+SPB | 0.020 | 1.09 | 0.45 to 1.73 | |||
| SPB+PSR [Normal] |
98.01 ± 12.96 | 90.84–105.19 | Baseline | <0.001 | 1.76 | 0.95 to 2.57 |
| Resting+SPB | <0.001 | 2.09 | 1.19 to 3.00 | |||
| Post PSR | <0.001 | 1.88 | 1.04 to 2.72 | |||
| Post SPB+PSR [Normal] | 81.58 ± 8.34 | 76.96–86.20 | Resting+SPB | 0.003 | 1.34 | 0.64 to 2.03 |
| PSR | <0.001 | -2.50 | -3.53 to -1.47 | |||
| SPB+PSR [Normal] | 0.001 | -2.34 | -3.31 to -1.36 | |||
| SPB+PSR [Pressure] |
99.26 ± 10.55 | 93.42–105.10 | Baseline | <0.001 | 2.39 | 1.39 to 3.38 |
| Resting+SPB | <0.001 | 2.83 | 1.70 to 3.97 | |||
| Post PSR | <0.001 | 2.73 | 1.63 to 3.83 | |||
| Post SPB+PSR [Normal] | <0.001 | 3.56 | 2.19 to 4.93 | |||
| Post SPB+PSR [Pressure] | 82.39 ± 8.54 | 77.66–87.12 | Resting+SPB | 0.001 | 1.46 | 0.73 to 2.19 |
| PSR | <0.001 | -2.64 | -3.71 to -1.57 | |||
| SPB+PSR [Normal] | <0.001 | -2.15 | -3.07 to -1.23 | |||
| SPB+PSR [Pressure] | <0.001 | -3.00 | -4.18 to -1.81 | |||
Note: Values are presented as mean ± SD with 95% confidence intervals. ANOVA results: F(7,98) = 66.95, p-value < 0.001, η2p = 0.83. PSR = pre-shot routine; SPB = slow-paced breathing.
| Condition | Mean ± SD | 95% CI | Significant Comparisons | |||
|---|---|---|---|---|---|---|
| Paired Condition | p-value | Hedges’g | 95% CI of g | |||
| Baseline | 40.02 ± 3.34 | 38.17–41.86 | - | - | - | - |
| Resting+SPB | 33.74 ± 2.12 | 32.56–34.91 | Baseline | 0.0001 | -2.27 | -3.23 to 1.32 |
| PSR | 47.94 ± 6.32 | 44.44–51.44 | Baseline | 0.002 | 1.38 | 0.67 to 2.08 |
| Resting+SPB | 0.0001 | 2.39 | 1.4 to 3.38 | |||
| Post PSR | 37.85 ± 4.86 | 35.16–40.54 | PSR | 0.0001 | -2.79 | -3.91 to -1.67 |
| Resting+SPB | 0.02 | 1.09 | 0.45 to 1.73 | |||
| SPB+PSR [Normal] |
46.35 ± 5.86 | 43.11–49.59 | Baseline | 0.006 | 1.26 | 0.58 to 1.94 |
| Resting+SPB | 0.0001 | 2.46 | 1.44 to 3.47 | |||
| Post PSR | 0.0001 | 2.41 | 1.41 to 3.41 | |||
| Post SPB+PSR [Normal] | 38.11 ± 4.07 | 35.85–40.36 | Resting+SPB | 0.0001 | 1.57 | 0.81 to 2.33 |
| PSR | 0.0001 | -2.24 | -3.18 to -1.29 | |||
| SPB+PSR [Normal] | 0.0001 | -2.72 | -3.82 to -1.62 | |||
| SPB+PSR [Pressure] | 46.14 ± 4.94 | 43.41–48.88 | Baseline | 0.002 | 1.39 | 0.68 to 2.10 |
| Resting+SPB | 0.0001 | 2.93 | 1.77 to 4.1 | |||
| Post PSR | 0.0001 | 2.96 | 1.79 to 4.14 | |||
| Post SPB+PSR [Normal] | 0.0001 | 3.49 | 2.14 to 4.84 | |||
| Post SPB+PSR [Pressure] | 38.21 ± 4.81 | 35.55–40.87 | Resting+SPB | 0.006 | 1.25 | 0.58 to 1.93 |
| PSR | 0.0001 | -2.40 | -3.4 to -1.4 | |||
| SPB+PSR [Normal] | 0.0001 | -2.67 | -3.75 to -1.59 | |||
| SPB+PSR [Pressure] | 0.0001 | -2.71 | -3.81 to -1.62 | |||
Note: Values are presented as mean ± SD with 95% confidence intervals (CI). ANOVA results: F(7,98) = 59.44, p-value < 0.001, η2p = 0.81. PSR = pre-shot routine; SPB = slow-paced breathing.
3.2. Effects on Swing Performance
As shown in Table 4, significant condition effects were observed for clubhead speed, total distance, and lateral deviation (p-value < 0.05). Post hoc comparisons indicated that values for these parameters were significantly higher in the SPB+PSR [Pressure] condition compared with the SPB+PSR [Normal], with moderate to large effect sizes (clubhead speed: Hedges’ g = 0.92, p-value = 0.008; total distance: Hedges’ g = 0.78, p-value = 0.024; lateral deviation: Hedges’ g = −0.82, p-value = 0.018). No significant differences were found between the PSR and other experimental conditions. Although the carry distance did not reach statistical significance, the highest mean values were observed under the SPB+PSR [Pressure] condition.
| Condition | Mean ± SD | 95% CI | Significant Comparisons | |||
|---|---|---|---|---|---|---|
| Paired Condition | p-value | Hedges’g | 95% CI of g | |||
| Clubhead speed (mph) | - | - | - | - | ||
| PSR | 107.77 ± 3.32 | 105.93, 109.61 | - | - | - | - |
| SPB+PSR [Normal] | 107.74 ± 3.10 | 106.02, 109.46 | SPB+PSR [Pressure] | 0.008 | –0.92 | -1.52 to -0.32 |
| SPB+PSR [Pressure] | 108.67 ± 3.36 | 106.80, 110.53 | - | - | - | - |
| Carry distance (yard) | - | - | - | - | ||
| PSR | 250.29 ± 10.55 | 244.45, 256.13 | - | - | - | - |
| SPB+PSR [Normal] | 250.79 ± 6.48 | 247.20, 254.38 | - | - | - | - |
| SPB+PSR [Pressure] | 253.98 ± 6.95 | 250.13, 257.83 | - | - | - | - |
| Total distance (yard) | - | - | - | - | ||
| PSR | 259.74 ± 10.45 | 253.95, 265.53 | - | - | - | - |
| SPB+PSR [Normal] | 260.13 ± 7.66 | 255.89, 264.37 | SPB+PSR [Pressure] | 0.043 | -0.78 | -1.26 to -0.14 |
| SPB+PSR [Pressure] | 263.97 ± 9.03 | 258.97, 268.97 | - | - | - | - |
| Lateral deviation (yard) | - | - | - | - | ||
| PSR | 16.57 ± 6.67 | 12.87, 20.26 | - | - | - | - |
| SPB+PSR [Normal] | 13.04 ± 5.54 | 9.97, 16.11 | SPB+PSR [Pressure] | 0.018 | -0.82 | -1.40 to -0.24 |
| SPB+PSR [Pressure] | 17.67 ± 5.95 | 14.38, 20.97 | - | - | - | - |
Note: Values are presented as mean ± SD with 95% confidence intervals (CI). ANOVA results: Clubhead speed F(2,28) = 4.27, p-value = 0.024, η2p = 0.23; Carry distance F(2,28) = 2.72, p-value = 0.083, η2p = 0.16; Total distance F(2,28) = 4.06, p-value = 0.028, η2p = 0.22; Lateral deviation F(2,28) = 4.20, p-value = 0.025, η2p = 0.23. PSR = pre-shot routine; SPB = slow-paced breathing.
3.3. Psychological Readiness before Swing Performance
The results showed a significant condition effect in all psychological components: mental clarity (χ2(2) = 12.45, p-value = 0.002), muscle relaxation (χ2(2) = 8.40, p-value = 0.015), and confidence (χ2(2) = 18.96, p-value < 0.001). Post hoc analysis showed significantly higher scores for the mental clarity factor under both SPB+PSR [Normal] (3.33 ± 0.49) and SPB+PSR [Pressure] (3.27 ± 0.59) compared to the PSR alone (2.40 ± 0.63, p-value < 0.05). Similarly, muscle relaxation scores were significantly higher in the SPB+PSR [Normal] (3.33 ± 0.49) than in the PSR alone (2.60 ± 0.63, p-value < 0.05). However, the SPB+PSR [Pressure] (3.13 ± 0.74) showed no significant difference compared to other conditions. Regarding self-confidence, the SPB+PSR [Pressure] condition showed significantly lower scores (2.33 ± 0.82) than both PSR (3.27 ± 0.59) and SPB+PSR [Normal] (3.33 ± 0.49; p-value < 0.05).
4. DISCUSSION
This pilot study examined the acute effects of integrating SPB into PSR on psychophysiological regulation and golf swing performance under normal and pressure-induced conditions and compared these responses across experimental conditions. The study's findings indicate that SPB-integrated routines enhanced vagal tone, psychological readiness, and specific performance outcomes compared with traditional PSR alone.
4.1. Psychophysiological Regulation and Cardiovascular Functions through Slow-paced Breathing
The study’s findings showed a significant increase in RMSSD during resting SPB and during integrating SPB+PSR under normal and pressure conditions. Although RMSSD was comparable to baseline, it remained elevated during the swings and was significantly higher than during PSR alone. The present study employed the SPB (4-2-8) technique, consistent with previous studies utilizing respiratory rates of 4–6 breaths·min−1 to enhance vagal tone and cardiovascular variability [15, 16]. This technique likely increases baroreflex sensitivity and respiratory sinus arrhythmia, thereby enhancing parasympathetic activity [7]. The increased vagal stimulation has been reported to reduce physiological stress and potentially mitigate anxiety [17, 18]. Notably, RMSSD remained similar across both normal and pressure conditions, suggesting that the SPB+PSR protocol may serve as a physiological buffer against autonomic arousal. Since our participants received psychological pressure intentionally induced by the researcher through performance evaluation, these might be relatively low to moderate in inducing psychological pressure and insufficient to suppress vagal activity. As noted in research on athletes, simulated pressure in training contexts may not reach the threshold required to suppress vagal activity, unlike high-stakes competition [19, 20].
Regarding cardiovascular responses, our results showed no differences in HR and %HRmax among conditions. However, participants demonstrated their lowest HR during SPB in seated rest, indicating the predominant effect of the parasympathetic system in the relaxation state [21]. The increased HR and %HRmax observed during golf swings were likely due to the physiological demands of muscle contraction and body movement, reflecting a low to moderate exercise intensity [22]. Other mechanisms, such as increased blood pressure and cardiac output during motor execution, may also contribute to these cardiovascular shifts [23]. Although HR and %HRmax increased above resting levels in all conditions, these changes showed less elevation in SPB+PSR conditions but exhibited the greatest increase during the PSR alone. These results suggested that SPB may counteract sympathetic cardiovascular responses during the golf swing, potentially buffering the stress response and enhancing swing performance.
4.2. Effects on Swing Performance
With respect to golf swing performance, performance outcomes were defined based on power (clubhead speed, total distance) and precision (lateral deviation). A distinct trade-off between these domains under varying arousal states was revealed by the findings. Under pressure, higher values for swing power were yielded in the SPB+PSR condition. It was suggested that the physiological arousal induced by the pressure condition, when regulated by SPB, may facilitate neuromuscular recruitment and force production [6]. Consistent with previous studies [7, 8], slow-paced breathing enhanced HRV and vagal tone, and slow-paced breathing stimulated changes in HRV and vagal tone, which directly corresponded with the physiological markers measured in the present study. Conversely, precision followed a distinct trajectory, illustrating a power-precision trade-off. While the SPB+PSR [Normal] condition exhibited the smallest lateral deviation, indicating superior directional accuracy. However, under pressure, lateral deviation increased despite the gains in power. These suggest that while SPB helps manage arousal, the sympathetic drive under pressure may prioritize force production over the coordination required for directional accuracy [24]. These outcomes may be explained by enhanced vagal tone and perceptual–motor integration during a low-arousal state, which promotes parasympathetic dominance and attentional stability [7]. Such findings highlight the necessity of balancing physiological activation with psychological control to ensure consistent performance.
4.3. Effects on Psychological Readiness
In the present study, results demonstrated an increased mental clarity and muscular relaxation in the SPB+PSR across both conditions, indicating a more relaxed and focused state prior to the golf swing. In line with previous research, slow-paced breathing has been shown to improve mental control in elite swimmers [25] and reduce pre-competition anxiety in competitive baseball players [26]. When facing stressful stimuli under pressure, the SPB protocol may regulate emotions by reducing negative feelings and high arousal, allowing golfers to remain focused during motor execution. Furthermore, the enhanced vagal tone and emotional stability driven by SPB appear to promote mental clarity and relaxation [27]. Nevertheless, golfers reported relatively low self-confidence scores during the SPB+PSR [Pressure] condition. These suggest that pressure may have negatively affected self-efficacy, as high stress can trigger a fear of failure, diminishing self-belief and confidence. Even with the physiological benefits of SPB, this decreased confidence may impair decision-making and ultimately reduce swing accuracy.
Taken together, the findings support the positive effects of SPB across psychological, physiological, and motor domains. From the results, the SPB+PSR intervention led to superior mental clarity and relaxation scores, with minimal HR increases and enhanced accuracy. These suggest that psychological readiness is closely linked to both autonomic regulation and motor consistency. Although golfers increased swing power under pressure, their shot accuracy slightly dropped alongside a reduction in self-confidence. These findings indicate that psychological stress may negatively impact confidence and precision despite stable physiological changes [28]. Consequently, the SPB intervention appears to be an effective strategy for regulating the psychological, physiological, and motor domains under high-pressure situations [10, 25].
5. LIMITATIONS
Although this study provided valuable evidence and insights into the integration of SPB into golfers' PSR, several limitations warrant consideration. Small sample sizes, consisting solely of male golfers aged 18–30, limited the generalizability of these findings to female players and different age groups. Additionally, the assessment of psychological readiness relied on single-item measures, which may limit both the reliability and construct validity of the data. Furthermore, this study focused only on immediate effects without evaluating the long-term learning, adaptation, or retention associated with the SPB+PSR protocol. Thus, future research should explore its long-term effects, adaptations across various skill levels, and integration into broader performance routines. Given that the pressure condition was induced through incentive-based ranking, this method may not fully capture the emotional complexity of actual tournament play. Consequently, future studies should employ a more diverse set of pressure stressors and assess performance consistency and error variability across repeated swings to better reflect the stability of psychological and motor responses across varying conditions.
CONCLUSION
Overall, the findings show that integrating Slow-Paced Breathing (SPB) into the Pre-Shot Routine (PSR) can serve as a practical tool for physiological regulation and mental clarity, improving physiological regulation, swing performance, and psychological readiness. While the SPB+PSR successfully enhanced vagal activity (RMSSD) under both normal and pressure conditions, its positive effects manifested differently across contexts. Under normal conditions, golfers were better at keeping the ball on target, preserving their directional accuracy. Although golfers felt less confident under pressure, the arousal generated resulted in a more powerful swing. When compared to a standard PSR, the SPB+PSR protocol offered more consistent psychophysiological advantages. As a simple and portable intervention, this protocol is ideal for high-precision sports, offering athletes a practical way to maintain physiological self-regulation while improving both mental focus and motor consistency.
AUTHORS’ CONTRIBUTIONS
The authors confirm their contributions to the paper as follows: A.T. and S.K.: Contributed to study concept and design, acquisition of data, analysis and interpretation of data, and administrative, technical, and material support; A.T., S.K., and S.S.: were involved in drafting the manuscript, critically revising it for important intellectual content, and supervising the study; A.T.: Performed the statistical analysis. All authors reviewed and approved the final version of the manuscript.
LIST OF ABBREVIATIONS
| HR | = Heart Rate |
| HRV | = Heart Rate Variability |
| PSR | = Pre-shot Routines |
| SPB | = Slow Paced Breathing |
| ms | = Milliseconds |
| %HRmax | = Percentage of Maximum Heart Rate |
| RMSSD | = Root Mean Square of Successive Differences |
ETHICS APPROVAL AND CONSENT TO PARTICIPATE
The study received ethics approval from the Ethics Review Sub-Committee for Research Involving Human Research Subjects of Thammasat University, Thailand (COA. 064/2565).
HUMAN AND ANIMAL RIGHTS
All human research procedures followed were in accordance with the ethical standards of the committee responsible for human experimentation (institutional and national), and with the Helsinki Declaration of 1975, as revised in 2013.
AVAILABILITY OF DATA AND MATERIALS
The data and supportive information are available within the article.
FUNDING
This study was supported by the Thammasat University Research Fund, Thailand Contract No. TUFT 34/2566.
ACKNOWLEDGEMENTS
We would like to extend our gratitude to the volunteer participants for their involvement in this study.

